He is a designated Certified Clinical
Densitometrist (CCD) by the International Society of
Clinical Densitometry
and our DXA Testing Center has
been approved by the Texas Department of State
Health Services as a Healing Arts Osteoporosis/Bone
Density Screening Site and accepts self-referrals
for DXA Bone Density Testing for clients that meet
certain criteria.
There are other screening machines
which look at the heel or forearm but unless you have had a
scan which looks at the L1-L4 Lumbar Spine, Bilateral Hips,
Bilateral Forearms and an Instant Vertebral Fracture
Analysis (IVA) you really don't know the status
of your bone health!!
Your results are compared to a young person
(approximately age 30) with maximum bone density
(T-Score) and with someone your age (Z-Score).
These scores indicate if you have decreased bone
density and will help predict your risk of future
fractures. Treatment decisions, in general are based
on the T-Scores, and in some cases the FRAX Plus Score
(see below). The World Health
Organization has defined "low bone density" (often
referred to as Osteopenia) as T-Scores of -1.0 to
-2.5 and "Osteoporosis" as T-Scores less than -2.5.
Z-Scores are used for men less than age 50 and
pre-menopausal females. Z-Scores less
than -2.0 are considered "below the expected range
for age" and Z-Scores above -2.0 are considered
"within the expected range for age".
The
Protocol for Clients Requesting DXA Bone Density
Testing
May
Include the Following Testing
Lumbar AP (Anterior Posterior)
L1-L4 & Supine Lateral L2-L4 Bone Density
Bilateral Hips (Both Hips are
Scanned and Analyzed)
Bilateral Forearms
(Both Forearms are Scanned and Analyzed)
High Definition AP & Lateral Instant
Vertebral Analysis (IVA) to look for vertebral
fractures
and Abdominal Aortic Calcifications
DXA Whole Body Composition
with Visceral Fat Analysis and
Calculation of
"low muscle mass" Indicies
Trabecular Bone Score Analysis of Lumbar Spine
FRAXplus Fracture Risk Analysis corrected by TBS
Score and/or Lumbar Spine T-Score
|
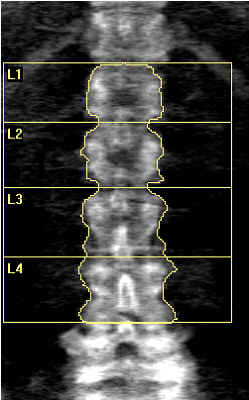 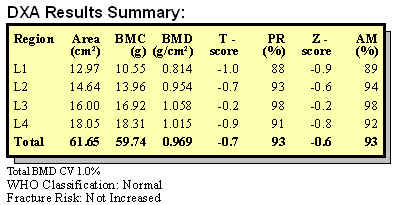
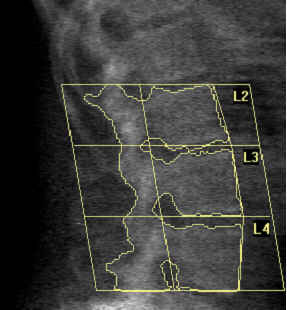
This is an AP DXA Scan of
the L1-L4 Vertebra in a 58 year old post
menopausal female. The Total T-score of -0.7
indicates normal bone density but there is
evidence of probable artifact elevation of
the measurements due to the sclerosis and
calcifications seen in the posterior
elements (Spinous Processes and Facet
Joints), so her true Bone Mineral Density is
probably lower. Lateral Views of the spine
might give a better measurement. Her Supine Lateral view of
the spine is below. |
|
 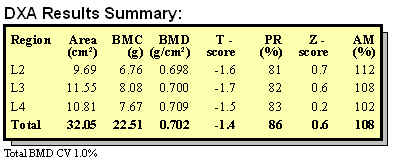
This is the Lateral DXA
Scan of the L2-L4 Vertebra only available on
a few DXA Scanners such as our Discovery A. These Lateral views
eliminate any artifact elevation of bone
density due to calcifications in the
posterior elements and give us a bone
density measurement of these vertebra
without any artifact. This study does
indeed show that this lady has lower bone
density
measurements in the L2-L4 vertebra which was
not apparent in the AP Exam. This
information might influence the treatment
program for this patient. The scanner also
allows for creation of detailed sampling
areas in the middle of these vertebral
bodies to get a more precise measurement of
the bone density in the interior of the
vertebra for following response to
treatment. |
Bilateral Hips (Both Hips are
Scanned and Analyzed)
|
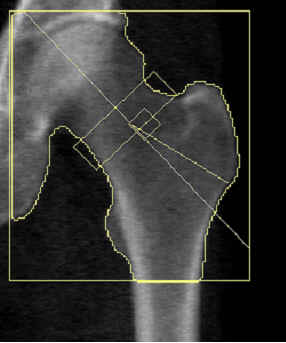 
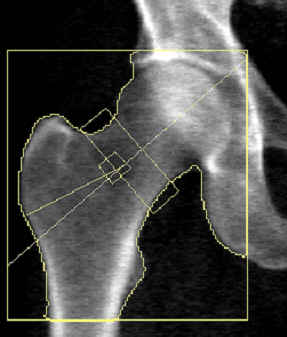
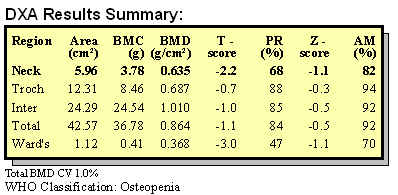
This is a DXA Scan of the
Left Hip in a 54 year old male which shows a
T-Score of -1.2 for the Total Hip and a
T-Score of -2.0 in the neck. This is a
definite diagnosis of low bone density of the Hip.
The Right Hip results are shown next.
|
|
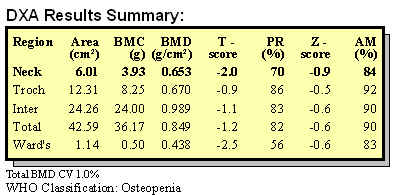
The Right Hip Scan shows a
T-Score of -1.1 for the Total Hip and a
T-Score of -2.2 in the Neck of the Right
Hip. The FRAX score discussed next uses the
lowest Neck Measurement to determine the 10
Year risk of a Hip or other Major
Osteoporotic Fracture. |

We will also calculate your
FRAX
Plus Score, a tool
developed by the University of Sheffield in 2008
to estimate your 10
year risk of either a Hip or other Major
Osteoporotic Fracture (vertebral, shoulder, forearm)
The risk
is based on the lowest T-Score of the Neck of the
Hip, where most fractures occur, your age, race,
country
and 7 questions about your medical history.
The FRAX results shown
are in the 54 year old male above and show the
influence of drinking
more than 3 units
of alcohol a day on the risk of a hip or other major
fracture. The New Frax Plus tool allows these
fracture risk
scores to be adjusted based on the L1-L4 Bone
Density and the Trabecular Bone Score.
|
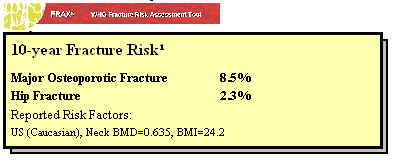 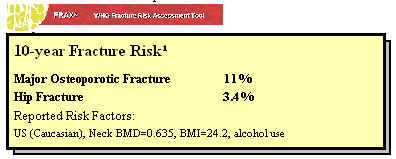
These FRAX Scores show the
10 Year risk of a Hip Fracture or other
Major Osteoporotic Fracture based on the
factors discussed above. It is
apparent that alcohol intake greater than 3
units per day markedly increases the 10 year
risk of a Hip Fracture from 2.3% to 3.4% and
the risk of a Major Osteoporotic Fracture
from 8.5% to 11%. This information might be
helpful in counseling a patient about this
particular risk factor. |
Bilateral Forearms
(Both Forearms are Scanned and Analyzed)
|
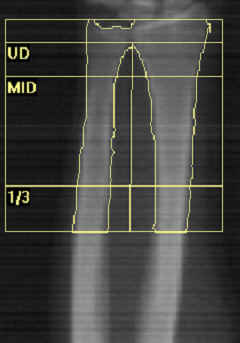 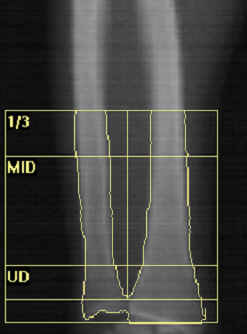
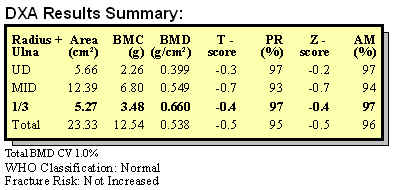
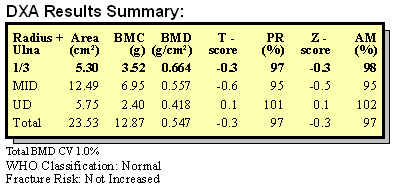
These
are the forearms scans of
a 24 year old Hispanic female with a history
of a eating disorder. The negative
T-scores show evidence that this young lady
has slightly lower bone density than females age 30
(T-Score) or females her age (Z-Score).
Women continue to develop their bone density
up until about age 30 so there still is time
to improve these measurements. Her T-Scores
and Z-Scores of the Femoral Necks and L1-L4
spine also showed that she was lagging
behind women age 30 and those her age.
Possibly, the
failure to achieve bone density equal to her
peers was
due to her dietary habits. This is a
bothersome trend that we are seeing more and
more as young women have increasingly bad
eating habits and eating disorders such as
anorexia and bulimia. These scores
can
improve with attention to nutrition
and exercise, but if not addressed, this
young lady may enter menopause without ever
achieving her maximum bone density as a
young adult. |
High Definition AP & Lateral Instant
Vertebral Analysis (IVA) to look for vertebral
fractures
|
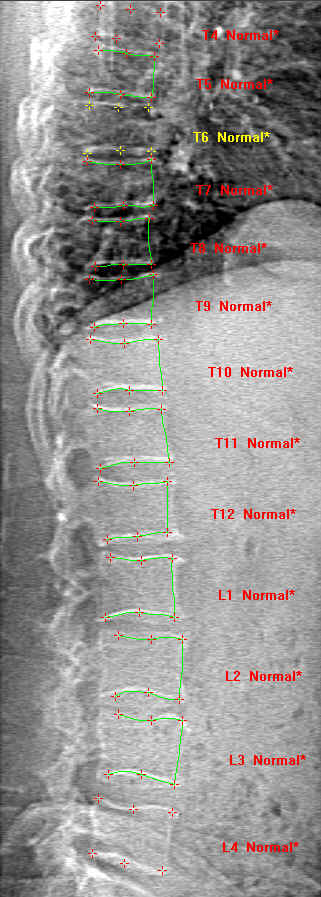 

The Horizon A Model
rotates and allows for both High Definition AP and
Supine Lateral Instant Vertebral Analysis of
the Spine to look for evidence of Vertebral
compression fractures which are sometime
silent but when present indicate a
significant level of loss of bone density.
Patients with these fractures are considered
to have a diagnosis of Osteoporosis and
should be treated to avoid future fractures.
The Hologic Software analyzes each vertebra
separately and can detect compression
changes.
The Lateral Scan can also
be used to detect Abdominal Aortic
Calcification which is an indication of
significant atherosclerosis and predictive
of future heart attacks and stroke.

See Detection of Abdominal Aoritic
Calcification with IVA
|
DXA Whole Body Composition Testing
|
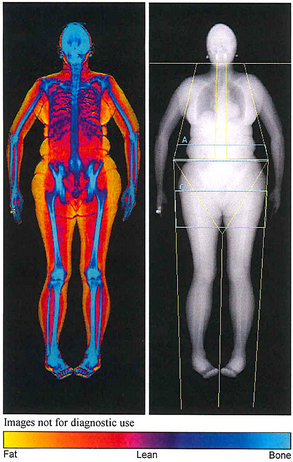 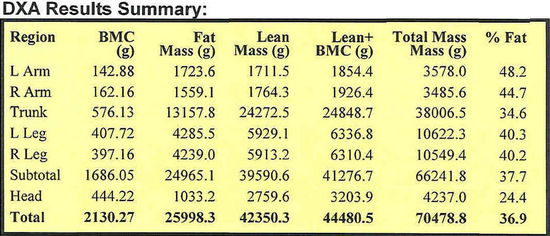
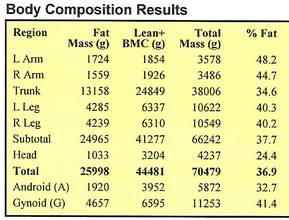
DXA Body Composition is a
research level tool and can be used to help
set goals for weight loss and gaining of
muscle. You can watch the yellow disappear
and the red increase. This
lady has a body fat % of 36.9%, too high for
her age.
See our
Modified Zone/Paleo Nutrition Prescription
and how we would combine it with
Hi-Lo Strength Training to
get the body fat % to 25%, much more reasonable for
a 58 Year Old female!! |

This is our
Fillable Intake .pdf Form for DXA Bone Density
Testing. It includes a Questionnaire to determine
your Risk Factors and must be completed prior to
your procedure.
Our DXA Body Composition
& Bone Density Brochure!
National Institutes of Health Web Site
Bone Health and Osteoporosis
A Report of the Surgeon General

In 2004 the Surgeon
General of the United States, Richard Carmona, issued
the first US Public Health Service report concerning Bone Health and Osteoporosis. It
was/is a sobering document which indicates that loss of bone
density is a much more serious problem that we have
previously thought and unless we change our eating and
exercise habits the problem will progress very rapidly.
Already, 10 million Americans
over the age of 50 have developed severe bone thinning or
osteoporosis; an additional 34 million have started down
that road and have an increased risk of fractures. To avoid
bone loss, Carmona’s report recommends getting the
recommended daily amounts of calcium from leafy green
vegetables, milk and cheese, and of Vitamin D; maintaining a
healthy weight and being physically active; and trying to
reduce the risk of falls. Ignoring the problem is expensive.
Americans spent as much as $18 billion on hospital,
physician and nursing home care to treat the 1.5 million
fractures attributed to osteoporosis in 2002. The cost could
double or triple in coming decades.
Update
Medicare White Sheet 2017 "Medicare Cost of Osteoporotic
Fractures)
Many people
think of osteoporosis as a disease of elderly women that
causes them to appear stooped over. These vertebral
fractures that cause the hunching over (called "dowager's
hump"), result in pain, loss of height, reduced lung
capacity and decreased exercise tolerance.
But this is only seen when the loss of bone
density is at its late stages.
We develop
our bone density between about age 13 and 30. After age
30, we all may lose our bone density at a slow rate.
Some people, especially young women and some men during adolescence
and young adulthood never
develop their maximum bone density. This can be due to
eating disorders such as anorexia, low calcium intake, too
many sodas/alcohol/smoking/vaping/drug use and sometimes due to too much exercise which
results in amenorrhea. Estrogen balance is disrupted when
amenorrhea occurs and bone formation is impaired. This is
called
The Female Athlete Triad, eating disorders, menstrual
disturbances and low bone mass.

In women, after menopause, the rate
of bone loss may increase. While most
fractures due to osteoporosis usually do not develop until
around age 65, osteoporosis has a long, quiet development
period when there are no symptoms at all. It is
important for young and middle aged adults to become aware of
osteoporosis while there is still time to prevent it.
Osteoporosis is not just a disease of women. Men account
for 20% of those with osteoporosis. Most people do not
know they have osteoporosis because there may be no symptoms
until they break a bone. By that time, the disease is
far advanced. Women with histories of dieting or eating
disorders early in life may never achieve maximum bone density
and unwittingly set themselves up for problems possibly in their
50's or early 60's.
After the scan we will spend about 30 minutes
going over the scan and your risk factors found on our
comprehensive
"Risk Factor Questionnaire". We have
found several young ladies in their 30's with early signs
of that their bone density is lower than others their age. In addition, men are not immune to loss
of bone density and many feel that this is a problem that is
under diagnosed in men. In our experience it
is rare to find normal bone density in a man who has a
very stressful lifestyle such as a professional or a
entrepreneur. These men with lots of stress in their lives
have many factors which impair bone health. Stress
lowers Testosterone and Growth Hormone levels which are good
for bones and raises cortisol levels which is bad for bone
health. In addition, these men often do not get enough
good restorative sleep when repair and growth occur. And to
make things worse, they don't exercise, eat poorly and may
smoke or drink too much alcohol. And we have yet to see a man
who takes a Calcium or Vitamin D Supplement regularly!!
We submit a detailed report for the referring M.D. and
the patient gets a copy of the report for their personal
records. We make recommendations for nutrition and exercise
strategies. We leave medical treatment decisions for
FDA approved drugs up to the referring doctor the patients
doctor of choice.
Our recommendations always include Hi Lo
Strength Training which was developed in part in the early 1980's by
Ken Hutchins, the founder of SuperSlow Strength Training. He was working with Nautilus at the time
and Nautilus was given the "Nautilus Osteoporosis Project"
and asked to design a strength training program for frail
seniors with osteoporosis. The Original Nautilus
Protocol was a 2 second Positive, 4 second Negative
repetition. The seniors were hurting themselves moving
the weights this fast, so Ken slowed it down to 10 seconds
up and 10 seconds down. The seniors could do this,
coaching was easier, they
got a lot stronger and bone density improved, however little
data was forthcoming due the the crude measurements of bone
density at that time. To quote Ken Hutchins "And
if we can assume the body to be logical then bone
strengthening should result from muscular strengthening"
It would make no evolutionary sense to allow the muscle to
get stronger and not allow the tendon and bone attached to
the tendon to get stronger at the same time. Since
aerobics does not reliably build strength or muscle mass, it
may not
the best choice to improve or maintain bone density.
EARLY
DETECTION of Bone Density Loss, TREATMENT with Hi-Lo Strength
Training and
proper nutrition, AND PREVENTION ARE OBVIOUSLY FAR BETTER
ALTERNATIVES THAN THE DISABILITY ASSOCIATED WITH THIS DISEASE.
Some common
osteoporosis risk factors include:
-
Estrogen deficient postmenopausal women
-
Caucasian or Asian Race
-
History of Fracture as an Adult
-
Maternal history of osteoporosis or other 1st degree
relative
-
High caffeine intake
-
Smoking/Vaping,
drug use and/or high alcohol consumption
-
History of eating disorder (Often seen in young women)
or malabsorption syndromes
-
Low calcium intake
-
Weight less than 127lbs
most of life
-
Athletic Amenorrhea
"Female Athlete Triad"
-
Inadequate physical activity
-
Chronic corticosteroid use,
even inhalers with steroids.
- High levels of Stress
- Any organ transplant or
autoimmune disease.
Resources



When
Should I be Scanned? My Opinion...FWIW
1.
Age 25-30 to identify women & men who may not have
achieved full bone mass density early in life if risk factors
are present.
2.
Age 40-45 to identify Bone Mass Status prior to Menopause. Men should get a baseline scan at this time.
3.
Age 50-55 to identify Bone Mass Status in the early post
menopausal years and to determine if there is increased
fracture risk.
DXA
Bone Density Testing
DEXA
Bone Density Testing